22nd Jul, 2021
With one-third of the world’s cases, India continues to bear the highest burden of tuberculosis globally and has been battling with the stigma of TB. Statistics reveal that TB kills an estimated 480,000 Indians every year and more than 1,400 every day. Apart from the “official” statistics, more than a million annual missing cases highlight that they go unreported or undiagnosed. Added to the health concerns of TB is the lack of knowledge about the disease and the social and economic ostracization that it brings with it. People tend to hide symptoms and do not seek treatment out of fear. There are many misconceptions related to TB, like it being incurable and even hereditary, adding to the challenge of its redressal.
India has had a rich tradition of panchayats. The modern Panchayati Raj Institutions (PRIs) institutions are based upon the belief that local development can be complemented by a robust local democracy, which holds authority over the local community and is a part of their lifestyles, cultures, and beliefs. PRI’s play a substantial role in the socio-economic development of people at the grassroots level. The role of PRI’s in responding to the challenge of TB is well documented. Various PRI’s work with different organizations, especially NGOs, using their resources and with minimal risks to assist them in combating the health menace of TB.
In 2011, the International Fund for Agricultural Development reported that 70% of the world’s 1.4 billion extremely poor live in rural areas. The majority of TB patients in rural areas live a life of poverty, severely limiting their options for diagnostics and treatment are severely limited due to lack of resources and money.
A WHO report stated that almost 50% of the world’s population lives in rural areas, but less than 38% of nurses and less than 25% of physicians work in these areas. TB patients who live in rural areas face a disadvantage when accessing even basic health care facilities. Studies have shown that patients also have to deal with limited and unpredictable clinic hours, long waiting and travel times, and frequent health provider absenteeism. Rural clinics are also more likely to face insufficient medication inventory compared to those in urban areas.
The scarcity of health facilities and the poor rural health infrastructure led to corruption and inefficiency. Even with free TB diagnosis and treatment policies, associated treatment activities like X-rays and prescription medicines, hospital admission, and time spent bear a cost to the patient.
Studies conducted across different zones have reported patients that have spent up to 40% of their annual income on TB-related health services. In addition, rural people might be unaware of their entitlements to treatment and are vulnerable to exploitation. People in rural areas battle the effects of stigma attached to TB, which prevents them from going for diagnosis or treatments. The stigma is so high that in many communities, patients refuse home treatment.
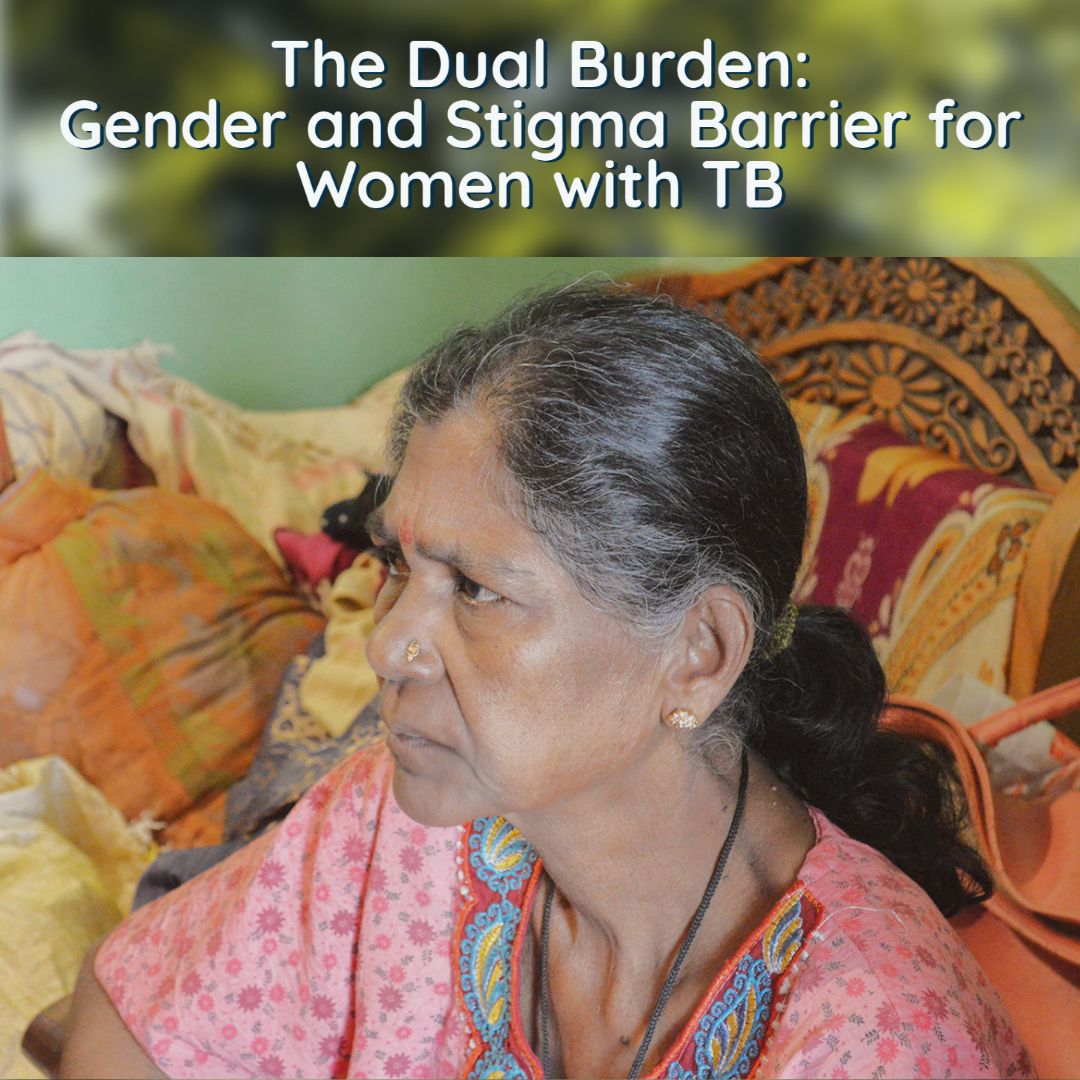
Women face longer delays in obtaining a diagnosis for TB due to social and cultural constraints. Women have also revealed that TB diagnosis could hamper their chances for marriage or damage their current relationships, thus making them more vulnerable.
The National Strategic Plan (2017-2025), launched by the Ministry of Health and Family Welfare, India, shows promise with the hopes of seeing new drugs, regimens, and diagnostics.
For the plan to succeed, it will require a concerted and active community engagement. Community involvement and local self-government bodies like Panchayati Raj Institutions can help combat some of the resistance and distrust often faced by the local populace. Panchayati Raj Institutions have deep connections and linkages with local people. PRI’s can enhance community-led early detection and treatment services.
The activities by the PRI’s will be supported by a high-visibility advocacy and communication program called “TB Mukt Bharat”. Periodic drives to identify and trace cases and offer TB preventive therapy to the identified populations will be implemented by seeking community commitment at the panchayat, district, and state levels. The TB control mission will closely monitor its implementation and performance. Socially and clinically vulnerable groups will be identified and mapped using available data from Municipal/ Block/ Taluka/
Zilla Panchayats records. The program will liaison with PRIs and other local government bodies through advocacy, communication, and community engagement. The policy advocacy should engage PRIs and local community leaders and educate them on the need for local action. Media advocacy can engage the local media to disseminate information. It is hoped that with strategic communication and social mobilization through PRI’s, community members will help in changing perception, behaviors, and practices among the local population.
TB is a global problem. It affects people in almost all areas, but it mainly affects rural regions across the world. It is therefore essential to understand the effects of poverty, malnourishment, and tobacco smoking on the prevalence of TB in India. Secondly, the public healthcare system is the lifeline of millions of Indians, and the gaps in it must be addressed on a war footing. The Revised National Tuberculosis Control Program is proactively working in this area. It has done some commendable work about providing free tests, drugs, treatment support, and the completion and involvement of private healthcare providers. There is, however, an immediate need to scale up a viable and effective delivery mechanism up to achieve the target of Zero TB in India by 2025. The PRIs can play an instrumental role in realizing this vision.
References:
1. https://tbcindia.gov.in/WriteReadData/NSP%20Draft%2020.02.2017%201.pdf
2. http://www.stoptb.org/assets/documents/resources/publications/acsm/kp_rural_spreads.pdf